
to learn more
government
other



➕ Financing
More government investment in primary health care is greatly needed, alongside more detailed data to better understand who is bearing the cost, where funds are coming from and how funds are being spent.➕ Capacity
Robust data collection on health system capacity is possible and necessary. By leveraging a mix of qualitative and quantitative data, country leaders have the best opportunity to uncover gaps that impact how a health system is functioning and act to improve primary health care.
➕ Performance
There is substantial room for improvement across access, quality and coverage of primary health care services; and quality remains the most under-measured dimension of primary health care performance, even after innovative efforts to fill data gaps through local sources.➕ Equity
Equity is a fundamental goal of primary health care. By comprehensively assessing the extent of disparities in access, coverage and outcomes within a health system, countries can pinpoint who is being left behind and progress further on their unique path to Health for All.


Creating an Evidence-Based Action Plan for Strong Primary Health Care
Ghana was among the first 11 countries to create a Vital Signs Profile and present it at the Global Conference on Primary Health Care in Kazakhstan in 2018. Just as meaningful as the results were the participatory processes that led up to and followed this moment — ultimately culminating in an evidence-based national Strategic Implementation Plan for PHC.
From the beginning of the Vital Signs Profile process, leaders at the Ghana Health Service emphasized the importance of Ghanaian stakeholders taking ownership at all levels, so that results could be institutionalized and woven into existing structures wherever possible. In order to make this happen, they convened a multi-stakeholder technical working group that drove the process of populating Ghana’s Vital Signs Profile to resonate in a local context, while PHCPI partners provided technical guidance and facilitation support.
Once completed, Ghana’s Vital Signs Profile reflected several key strengths of the health system, drawing on decades of investment in primary health care. For example, Ghana stood out for having a clear cadre of health workers who were adequately trained, salaried, and distributed across the population, and whose primary responsibilities were primary health care-related – just one important legacy of Ghana’s trailblazing Community-based Health Planning and Services (CHPS) program, established in the 1990s.
The Vital Signs Profile also demonstrated several key areas for improvement, including ensuring clear management structures at the facility level and tracking the supply of essential medicines and equipment.
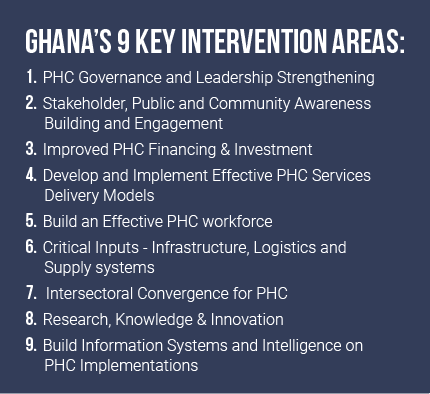
These Vital Signs Profile results were put to work right away. With support from a Trailblazer Opportunity Fund grant from PHCPI, Ghana’s Vital Signs were distributed widely to stakeholders at national, regional, district, and health facility levels. This helped set the scene for regional workshops with 70+ Senior Managers to define priorities for a national Strategic Implementation Plan for primary health care. According to key stakeholders, the process of completing and disseminating the Vital Signs Profile played an important role in sensitizing key decision-makers to the ‘health’ of primary health care in Ghana; building consensus on key strategies to fix gaps; and informing the nine top priorities for the Strategic Implementation Plan (see box) – each coupled with short, medium, and long-term actions.
At the end of the day, countless stakeholders later commented that the participatory process for producing and leveraging the Vital Signs Profile was as valuable as the results, generating significant stakeholder engagement and buy-in that enabled a rigorous understanding and snapshot of primary health care in Ghana to be embraced and translated to action.
Aligning Public & Private Health Care Systems to Meet People’s Needs
After completing a partial Vital Signs Profile in 2018, the Malaysian Ministry of Health decided to collect data on Capacity measures by completing a PHC Progression Model in 2020. They wished to continue improving comprehensive measurement of primary health care in Malaysia, including for quality of care; and to increase Malaysia’s ability to benchmark and showcase its progress on a global scale.
The Ministry of Health also brought specific questions to the table – namely, how to better understand and integrate the country’s public and private health care systems.
Like many countries, Malaysia offers primary health care services through both public and private providers, with around 3,000+ public facilities and 6,000+ private facilities. Even though there are more private facilities across the country, the public sector accounts for approximately 64% of primary health care utilization in the country. The public sector is heavily subsidized by the government, whereas the private sector charges user fees for patients.
The Progression Model highlighted that information systems are one particular strength of Malaysia’s public health sector, from successfully recording 90-99% of all births and deaths in the country to maintaining long-term personal care records in 91% of public health clinics. Malaysia also regularly collects health status updates from all public primary health care facilities. Beyond informing direct patient care and administration in communities, this facility data feeds into a centralized Malaysian Health Data Warehouse that supports strong governance and informed planning at the national level.
By comparison, Malaysia’s private sector facilities were not as integrated into the country’s information systems. If harnessed to support the private sector as well, these systems could help boost quality and responsiveness across all facilities.
The Ministry of Health was committed to including a close look at the private sector in its Vital Signs Profile assessment. The Progression Model enabled the MOH to unearth specific, actionable information, including:
- Exactly where and how many private facilities did not have data integrated into existing information systems
- Which facilities have regulatory approval to deliver essential drugs or required, well-functioning equipment.
Now, the government is exploring ways to address remaining data gaps and strengthen coordination with the public and private sectors, building on the recent launch of a web-based platform to facilitate data collection from private practitioners. The country will review current legislative instruments like the Private Healthcare Facilities & Services Act and assess the potential for expanded use of electronic medical records, surveys, and audits to further institutionalize data collection from the private sector.
The upcoming National Policy for Quality in Healthcare, expected to launch in October 2021, will also reflect additional pathways to strengthen engagement between both sectors to strengthen primary health care delivery.
Strengthening Local and National Information Systems during COVID-19
In the last year, Mozambique completed its Vital Signs Profile amid the COVID-19 pandemic. The Ministry of Health quickly leveraged assessment results to develop the country’s 2020-2024 Strategic Plan for the Health Sector. While the previous strategic plan for 2014-2019 was grounded in the guiding principles of primary health care, it lagged in the use of evidence and data to inform and implement concrete policies and plans to strengthen the health system. The Vital Signs Profile data, including the Progression Model, helped bring areas for improvement into sharp focus and shape an array of primary health care initiatives—from crafting new health sector policies to formulating investment plans for the Global Fund and Global Financing Facility.
Mozambique was able to draw on a uniquely rich set of data to complete its Vital Signs Profile, particularly at the sub-national level, due to efforts to develop resources like Community Score Cards and Performance Balance Reports that are used in 75% of districts and 75% of health facilities. This helped government stakeholders to clearly identify and track goals across national, provincial, and district levels. Critically, the Vital Signs Profile identified that at all levels nationwide more investment is needed in the fundamental building blocks of primary health care – elements such as the availability of essential medicines, basic equipment, and the health workforce.
Data also revealed key differences between levels of the health system in resources for and implementation of primary health care. Identifying these gaps has been instrumental as Mozambique continues work to decentralize administrative and financial governance of the health system. The country was able to act quickly to address one key gap in the use of informational systems to respond to the COVID-19 pandemic. Though Mozambique has an electronic monitoring and evaluation system, the Progression Model revealed it was not being fully implemented in lower, community-level facilities. Limited analytical capacity and a reliance on paper records in most health centers contributed to poor data quality, undermining the ability of the system to support effective decision-making.
This insight influenced Mozambique’s decision to roll-out a novel surveillance system at community-level facilities to capture flu-like symptoms as part of the national COVID-19 response. Local focal points were appointed to capture and transcribe COVID-19 indicators into the national database, providing more timely and complete information to support the Ministry of Health in COVID-19 response planning and resource allocation.